
To decrease patients postoperative ’ nausea and vomiting by using aromatherapy as a comfort measure in addition to antiemetic medications.
DATE: February, 2025
This evidence-based practice (EBP) project aims to implement a hospital grade essential
oil blend to decrease postoperative nausea and vomiting (PONV), post anesthesia care
unit (PACU) length of stay, and overall antiemetic/anti-nausea medication use, ultimately
improving patient outcomes and satisfaction in the women’s services department and
decreasing costs. Additionally, it aims to increase uninterrupted maternal/infant bonding
through skin-to-skin contact, aligning with a patient-centered care model.
AUTHORS
Morgan Fischer, BSN, RNC-OB, C-EFM
Labor & Delivery, Women’s Assessment Center , OB Critical Care & Transport
Sharon M. Burks MSN, RNC-OB, C-EFM
Assistant Clinical Director, Labor & Delivery, Women’s Assessment Center, OB Critical Care
& Transport
BACKGROUND
PONV is a commonly known side effect from the use of anesthesia and undergoing both
OB and GYN surgeries in the adult women’s services population. Current nursing practice
includes giving medications such as ondansetron and promethazine, and to prevent and
treat PONV (Gan et al., 2020). While beneficial, these medications can also cause unpleasant
side effects such as headaches, constipation, extrapyramidal symptoms, and more (Gan
et al., 2020). PONV can lead to an increase in medication use, increased interruption
in maternal/infant bonding as skin-to-skin contact is difficult when a patient is vomiting
or drowsy, incisional pain from vomiting, delay advancing diet, delay PACU discharge,
increased hospital costs, and can decrease patient satisfaction.
The use of therapeutic inhaled essential oils, as an effective non pharmacological
therapeutic treatment option, is quickly gaining acceptance in the acute care setting.
There is a strong body of evidence to support the positive effects essential oil blends can
have on PONV in decreasing the need for additional doses of antiemetics/ anti-nausea
medications postoperatively. Literature supports the nursing practice of using essential
oils as an additional method to reduce PONV, reduce antiemetics/anti-nausea medication
usage, reduce postoperative recovery costs, improve outcomes, and positively affect patient experience (Asay et al., 2019; Fearrington et al., 2019; Trandel-Korenchuk et al., 2020).
RELEVANCE/SIGNIFICANCE
Postoperative nausea and vomiting accounts for a significant amount of the delays in PACU discharge in the hospital’s women’s services department at a large, academic hospital. Antiemetic/anti-nausea medication costs and delays in PACU discharge also contribute to a financial burden on the hospital. A team led by a labor and delivery staff nurse identified TIEO as an evidence-based practice initiative. The inclusion criteria for this initiative included non-gravid, female assigned sex at birth, post-op cesarean section or gynecological patients with PONV. Exclusion criteria included patients under 18 years of age, gravid patients, and patients with allergies or aversions to essential oils. The following outcomes pre and post-implementation were used for evaluation:
- Postoperative Nausea and Vomiting score
- PACU length of stay
- Antiemetic/Anti-Nausea medication use
- Skin-to-skin contact time
- Patient satisfaction with intervention
Project evaluation results will be reported to department leadership and hospital Evidence-
based Practice and Research Council to assess the feasibility for implementation and
expansion to other units within the hospital system.
STRATEGY/IMPLEMENTATION/METHODS
This evidence-based practice initiative team was made up of nine nurses from the
unit’s professional governance council. This team utilized the Johns Hopkins EBP
Model to guide this initiative. For this initiative, the following PICOT question was
developed: (P) For non-gravid female assigned sex at birth post-op c-section or GYN patients with post-op N/V (I) how does Therapeutic Inhaled Essential Oils (TIEO) (C), when compared to anti-emetics or anti-nausea medication, as a first line to treat PONV (O) improve patient reported PONV (T) at time of discharge. This PICO question guided the literature review that yielded over 100 articles of which 15 were critically appraised. Upon the evaluation of evidence, the nurse-led team confirmed the implementation of TIEO as an evidence-based practice for implementation. Once the PICOT question and literature review were completed, the nursing team was guided by a co-nurse investigator, the Director of Nursing Excellence & Inquiry, to complete a logic model to define short-, intermediate-, and long-term outcomes. Data collection involved a retrospective chart review and voluntary patient surveys in English and Spanish. Additionally, the nurse-lead team collaborated with the physician department heads and anesthesiology to collaboratively plan for change management and to foster
interdisciplinary support.
A hospital approved vendor was selected and a total of 210 samples of the Joint Commission approved TIEO product were received from the vendor free of charge. To ensure ethical standards were met, the EBP study was evaluated by the organization’s IRB of record and received a determination that the activity does not constitute as human subjects research. The primary nurse investigator completed CITI training and continued to perform duties as a staff nurse for the duration of this project to mitigate conflict of interest. This TIEO product included a 100% natural and premium quality essential oil blend of mentha piperita (peppermint), mentha spicata (spearmint), lavandula (lavender), and zingiber officinale (ginger). The product comes in a peel pack and clips onto a patient gown. Once a patient
received the TIEO product, it stayed with them throughout their hospital stay and was sent
home with the patient at time of discharge.
In preparation for this initiative, the team provided staff and patient education. Patients
were evaluated for PONV using a standardized PONV descriptor scale that is part of the
EPIC recovery flowsheet. After scoring, if the patient requested intervention for PONV
the nurse offered TIEO while obtaining antiemetic/anti-nausea medication. TIEO did not
replace medications; it was used in combination or independent of medications. If the
TIEO alleviated the patient’s PONV within 3-5 minutes of use, then there was not a need to
give the antiemetic/anti-nausea. RN assessed patient’s reported need for pharmacologic
intervention prior to administration. If nausea persisted after using TIEO, then the
medications were given as ordered. Per standard work, the RN scored patient’s PONV in the recovery flowsheet after intervention and prior to discharge of PACU. “Aromatherapy” was added to the EMR nursing flowsheet for nurse intervention documentation. Patients that elected to use TIEO as an intervention were given a voluntary anonymous survey at time of discharge via Microsoft Forms.
The intervention took place over a 10 weeks period, 9/4/2024-11/14/2024 until the 210
TIEO samples were completed. Retrospective data analysis was conducted by the nurse
team to gather project results and measure clinical outcomes. Results will be presented to department leadership and the hospital’s Evidence-Based Practice and Research Council to assess the feasibility of expanding TIEO as a first-line nursing intervention for PONV across other hospital units.
EVALUATION/OUTCOMES/RESULTS
The intervention aimed to decrease PONV, PACU length of stay, and overall antiemetic/
anti-nausea medication use, in the women’s services department. Additionally, it aimed to
increase uninterrupted maternal/infant bonding through skin-to-skin contact. This project is also in the process of being analyzed for a potential reduction in healthcare costs associated with additional mediations and PACU delays.
Data analysis utilized both primary and secondary datasets. Primary data included EMR reports on LOS, PONV scores, and skin-to-skin contact duration. Secondary data consisted of qualitative feedback from patient and staff surveys. All data was deidentified for confidentiality.
A postoperative nausea and vomiting verbal descriptor score was documented by nursing
staff 5,423 times in the pre-intervention PACU period. The average PONV score for this pre-intervention period was 0.42. This PONV verbal descriptor score was documented by nursing staff 4,988 times in the post-intervention PACU period. The average PONV score for this postoperative period was 0.49. Nurses were instructed to document the TIEO intervention as “aromatherapy” for this project. A total of 50 charts were found in the EPIC search with “aromatherapy” documented as the PONV nursing intervention during the PACU period. These 50 charts were audited individually for pre- and post-intervention PONV verbal descriptor scores. It was discovered that there is a wide variation in the frequency of nurse assessment and documentation of PONV scores. For example, one nurse charted the PONV verbal descriptor score as 0 (x11) prior to a score of 5. Once the patient showed signs of PONV, the nurse administered TIEO and then the reassessment PONV verbal descriptor score was 2. The numerical score went down from 5 to 2, showing improvement in patient symptoms. Another patient’s PONV verbal descriptor score prior to receiving TIEO was charted as 0 (x20), 1, 0, 0, 6, 4 respectively. After the patient received TIEO, the reassessment scores were 3 and 0 respectively. When taking an average of the scores pre-and post-intervention, the extra scores of zeros charted pre intervention make it difficult to measure the statistical significance of this intervention. The clinical significance showed an improvement of PONV symptoms in both of these cases.
In the Main OR PACU, approximately 163 samples reflected positive outcomes, with a 3.6% decrease in PACU LOS for cases with recovery times greater than zero minutes (712 pre implementation, 718 post implementation).

In the L&D PACU, approximately 47 samples reflected areas of opportunity and showed a 7.2% increase in PACU times post implementation (295 cases pre implementation, 204 cases post implementation). Contributing factors included hospital construction disruptions, varied PACU locations, and competing priorities such as initiatives to reduce cesarean section rates. Future improvements may involve dedicated intrapartum products and enhanced staff education.

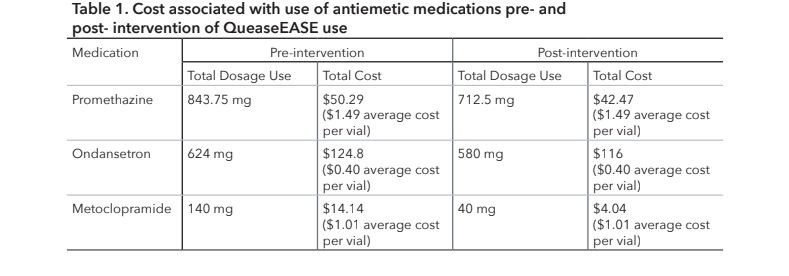
The sum of total milligrams of ondansetron (Zofran), promethazine (Phenergan), and metoclopramide (Reglan) administered in the PACU period pre-intervention (n=187 nurse medication documentations) was compared to the sum of total milligrams post-intervention (n=183 nurse medication documentations). A general medication cost list from EPIC was also provided and an average of each medication was calculated. This price value was then used when calculating price per dose and total cost.
Skin-to-skin contact charted as initiated during cesarean PACU recovery increased slightly from 44.2% of admissions pre-implementation to 45.1% of admissions post-implementation. Patient surveys (n=43) indicated high satisfaction, with 98% affirming the essential oils’ effectiveness in reducing nausea and willingness to use them again. Comments emphasized the oils’ efficacy in alleviating nausea, reducing anxiety, and providing a calming sensory experience. Some patients noted immediate symptom relief and expressed a preference for natural remedies, though a minority found the scent polarizing.
A sample size of 210 TIEO products also limited the scale of this project. Next steps for the intervention include developing a new organizational system and ensuring sustainability of the restocking process by ordering supplies through the system. Additional training for staff on postpartum and antepartum units are needed to reinforce the use of TIEO past the immediate PACU period and increase cohesion of the treatment of PONV among the different units.
PACU nurses reported positive experiences with the intervention, noting its utility for pre-and post- operative nausea and anxiety management. A recurring theme among L&D nurses was the need for similar products tailored to intrapartum and postpartum use, reflecting the intervention’s broader applicability.
CONCLUSIONS/IMPLICATIONS FOR PRACTICE
This project demonstrated the potential for TIEO as an effective, patient-centered intervention for managing PONV and pre-/post-surgical anxiety. Nursing leadership, physician department heads, and anesthesia teams expressed strong support, reflecting the alignment of this initiative with evidence based practice and transformational leadership principles. It is recommended that the use of TIEO should be continued as the first line nursing intervention for PONV to promote optimal patient health and wellness. Project evaluation results will be reported to department leadership and hospital Evidence-based Practice and Research Council to assess the feasibility for implementation and expansion to other units within the hospital system. The 3.6% reduction in PACU times in the main OR suggests that TIEO contributed positively to operational efficiency. Although the analysis of maternal-infant bonding through skin-to-skin times showed no statistically significant improvement, further exploration with refined methodologies may better capture TIEO’s impact on this outcome. Patient surveys revealed overwhelming approval, with 98% of respondents rating TIEO favorably for nausea and anxiety management, highlighting its popularity and patient-centered nature. A decrease in overall antiemetic and anti-nausea medication usage in the post intervention PACU recovery phase also supports the use of TIEO to decrease the unwanted symptoms of PONV, unwanted side effects of medication usage, and decrease associated hospital medication costs. This low risk, high benefit nursing intervention has been greatly received by both the patients and staff caring for those patients in the PACU and recovery setting and should be incorporated as the standard of nursing care for treating PONV. Furthermore, studies should be done to explore the use of TIEO to decrease nausea in the intrapartum phase of labor as this was highly requested by the labor and delivery nurses.
REFERENCES
Asay, K., Olson, C., Donnelly, J., & Perlman, E. (2019). The use of aromatherapy in
postoperative nausea and vomiting: A systematic review. Journal of PeriAnesthesia Nursing,
34(3), 502–516. https://doi.org/10.1016/j.cnur.2020.06.015
Fearrington, M. A., Qualls, B. W., & Carey, M. G. (2019). Essential oils to reduce postoperative
nausea and vomiting. Journal of PeriAnesthesia Nursing, 34(5), 1047–1053. https://doi.
org/10.1016/j.jopan.2019.01.010
Gan, T. J., Belani, K. G., Bergese, S., Chung, F., Diemunsch, P., Habib, A. S., Jin, Z., Kovac,
A. L., Meyer, T. A., Urman, R. D., Apfel, C. C., Ayad, S., Beagley, L., Candiotti, K., Englesakis,
M., Hedrick, T. L., Kranke, P., Lee, S., Lipman, D., … Philip, B. K. (2020). Fourth Consensus
Guidelines for the management of postoperative nausea and vomiting. Anesthesia &
Analgesia, 131(2), 411–448. https://doi.org/10.1213/ane.0000000000004833
Trandel-Korenchuk, S. C., Gujral, H., Bode, C., & Bindon, S. L. (2022). Aromatherapy blend
for postoperative nausea in ambulatory surgery patients. Journal of PeriAnesthesia Nursing,
37(1), 19–23. https://doi.org/10.1016/j.jopan.2021.01.003